


Nurses Need Our Help, and PBMs, and CONs
A free public service for a better community


A Good Day To Advocate for Better Healthcare
If there are subjects you’d like to see or improvements made, please let me know using the comment button below. Videos of these newsletters appear on Youtube on this channel. Let me know what you think.
Pharmacy Benefit Manager (PBM) Reform?
A House panel passed a bipartisan bill to ban drug middlemen from charging fees based on drug list prices — the first in Congress’ raft of PBM reform efforts that would actually ban the practice in at least some of the employer-sponsored insurance market. I checked the text of the bill and found it hard to determine to which insurance plans it applied
The bill, H.R. 6283, by Rep. Mariannette Miller-Meeks (R-Iowa), would only allow PBMs to charge a flat service fee, separating those fees from list prices. The bill also would ban the PBM practice, called spread pricing, of charging insurers more than they pay pharmacies. And it would prohibit PBMs from steering patients to pharmacies affiliated with them.
It is a start, but the real answer is - right - Universal Healthcare. That would give us the ability to negotiate fair prices with drug makers, without a pharmacy benefit manager standing in the middle taking bribes.
Nurses at Risk
Nearly half of nurses reported an increase in workplace violence last year, leading many to consider leaving their job or healthcare altogether, according to a recent survey from National Nurses United. The survey gathered data from more than 900 nurses nationwide and found that in 2022 and 2023 more than 80% of nurses experienced some form of workplace violence. Attacks ranged from bites, punches, kicks and thrown urinals to “racist and sexually aggressive comments,” the union said.
Eight in 10 nurses (81.6 percent) have experienced at least one type of workplace violence within the past year.
Nearly half of nurses (45.5 percent) reported an increase in workplace violence on their unit in the previous year. In contrast, only 3.8 percent of nurses reported that workplace violence has decreased on their unit in the previous year.
Nurses experience multiple types of workplace violence on a daily basis, ranging from physical abuse to verbal threats. The three most common types of violence reported were being verbally threatened (67.8 percent), physically threatened (38.7 percent), and being pinched or scratched (37.3 percent).
To read the full report, including statistics and sources, go here.
The Workplace Violence Prevention for Health Care and Social Service Workers Act (S. 1176/H.R. 2663) is aimed at protecting nurses, other health care workers, and their patients from workplace violence. These federal bills would mandate that federal OSHA create a standard that would require health care and social service employers to create, implement, and maintain effective workplace violence prevention plans. Under S. 1176/H.R. 2663, such a standard would include all the elements that effectively protect nurses and other health care workers. While we are at it, Congress should implement safe levels of staffing for nurses as well as in the Nurse Staffing Standards for Hospital Patient Safety and Quality Care Act of 2023 (S. 1113/H.R. 2530). P.S. Safe staffing for nurses is also a part of proposed universal healthcare, H.R. 3421, the vastly improved Medicare for All Act. I’m just saying.
Let’s ask Congress to get in gear and make hospitals a little safer for those that are there to help us. Part of that is to set safe staffing levels for nurses as well.
ACTION
Let your member of Congress and Senators know that nurses need a safe place to work and that they should pass The Workplace Violence Prevention for Health Care and Social Service Workers Act (S. 1176/H.R. 2663) and S. 1113/H.R. 2530, the Nurse Staffing Standards for Hospital Patient Safety and Quality Care Act of 2023. Contact info for them is in the References section below.
Or you can use RESISTBOT on your cellphone and text SIGN PWOCBJ to 50409 to send the email below.
“I am your constituent and I just learned that according to a National Nurses United Union study over 80% of nurses have been subject to workplace violence. They help us and now they need our help. I want you to do two things for them.
First, I want you to cosponsor and pass S. 1176/H.R. 2663, the Workplace Violence Prevention for Health Care and Social Service Workers Act so that OSHA creates a standard that would require health care and social service employers to create, implement, and maintain effective workplace violence prevention plans.
Second, I want you to cosponsor and pass the Nurse Staffing Standards for Hospital Patient Safety and Quality Care Act of 2023 (S. 1113/H.R. 2530) so we don’t overwork nurses and risk patient health outcomes. Of course, if you would just pass H.R 3421, the vastly improved Medicare for All Act - these safe staffing levels would be in place. Thank you.”
Certificate of Need Programs
A reader asked me information on Certificate of Need programs yesterday. Here it is.
Certificate of Need (CON) programs primarily aim to control health care costs by restricting duplicative services and determining whether new capital expenditures meet a community need. A good reference is this Investopedia.com article.
A certificate of need (CON) is a legal document that is required in order to construct a new healthcare facility. A developer of a healthcare facility must demonstrate why the community would benefit from that new development. The criteria used to evaluate the application can vary by location. 35 states and Washington DC require them. See Certificate of Need (CON) State Laws.
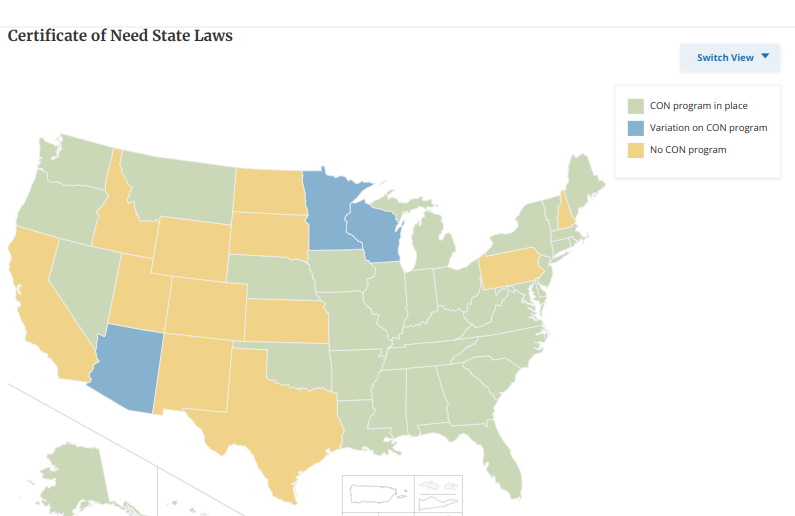
In the above map you can see which states still have certificate of need programs.
Pros and Cons
Critics say the system poses an unnecessary barrier to entry in the healthcare market, effectively protecting established health facilities from competition.
The earliest such laws appeared in the mid-1960s, with New York adopting the first such statute in 1964. In 1974, the Federal Health Planning Resources Development Act was passed. It offered states a financial incentive to pass Certificate of Need programs. Such incentives stopped in 1987. There has been an effort underway for several years to modernize these rules.
Traditionally, advocates for the CON framework contend that they help prevent unnecessary spending on healthcare infrastructure and services, and that they can help states to direct such infrastructure toward underserved regions.
Critics, on the other hand, argue that the CON framework protects the interests of established facilities. These critics also argue that, by allowing political influence to decide which facilities can be built, the CON system invites corruption, manipulation, and abuse.
In 2023 Connecticut, North Carolina, Virginia, Washington and West Virginia all modified their CON programs in various ways. For example, Washington exempted CON review for kidney disease centers during temporary emergency situations and West Virginia exempted birthing centers from CON review.
Here is a link to the National Conference of State Legislatures site. The states are all listed and if you select one the details of the Certificate of Need program (if any) in that state is presented. For instance, in my state, Washington, there is now an exemption for psychiatric hospitals (I guess we need more of those). In Washington CONs apply to hospitals and hospices. As an aside, it is not a bad idea to apply it to hospices since that is an area that is rife with fraud. I’ve written about that fraud here.
I also discovered that in Washington, there are 19 bills before the legislature, right now, addressing certificates of need. One of them HB 2128 seeks to modernize the program and would authorize a commission to determine the effect of such programs in the state.
Here is a link to the Washington State Certificate of Need Program so you can see how they administer it.
RESOURCES
Healthcare Advocacy (Us)
Website
Our Newsletter resources including reproductive healthcare
Healthcare Advocacy Reading List
Find My Elected Officials
Contact the White House https://www.whitehouse.gov/contact/
Contact State and Federal Representatives
By phone: (202) 224-3121
By email: democracy.io
Important Healthcare Resources
League of Women Voters Healthcare Reform Toolkit
Organizations to Contact
National Nurses United Medicare4All
Physicians for a National Health Program
One Payer States
Healthcare Now
Reproductive Health
NARAL - Pro Choice America
Charley. chatbot abortion resource - make sure to use a secure incognito browser if you live in a state that has banned abortion
Planned Parenthood
Miscarriage and Abortion Hotline has references about where to procure abortion medications. They also assist women in the process of self managed abortion or miscarriage by phone or text and will respond in an hour. Details and hours of operation at their website.
United State of Women Reproductive health page (bottom of the page) has important resources such as medical support, access to Telehealth, prescriptions by mail, and legal support references.
Practice careful communications - The Digital Defense Fund has a number of tips to keep texts, calls, and internet use private. Here is their site.
If you need financial help with an abortion try abortionfunds.org
Claims Denials and Appeals & What to Do
Appeal a Healthcare Decision
Appeal/Negotiate a Hospital Bill
Disinformation Management
Cybersecurity Infrastructure Security Agency
Save Democracy
Chop Wood, Carry Water by Jessica Cravens
RESISTBOT
Link to the RESISTBOT site to learn more
Link to Chop Wood, Carry Water RESISTBOT write up
Thanks for reading Healthcare Advocacy! Subscribe for free to receive new posts